As research advances in autoimmune and inflammatory disorders, we are learning that diseases within this broad spectrum—triggered by either external or internal stimuli—disproportionately affect women. This manifests in two different ways:
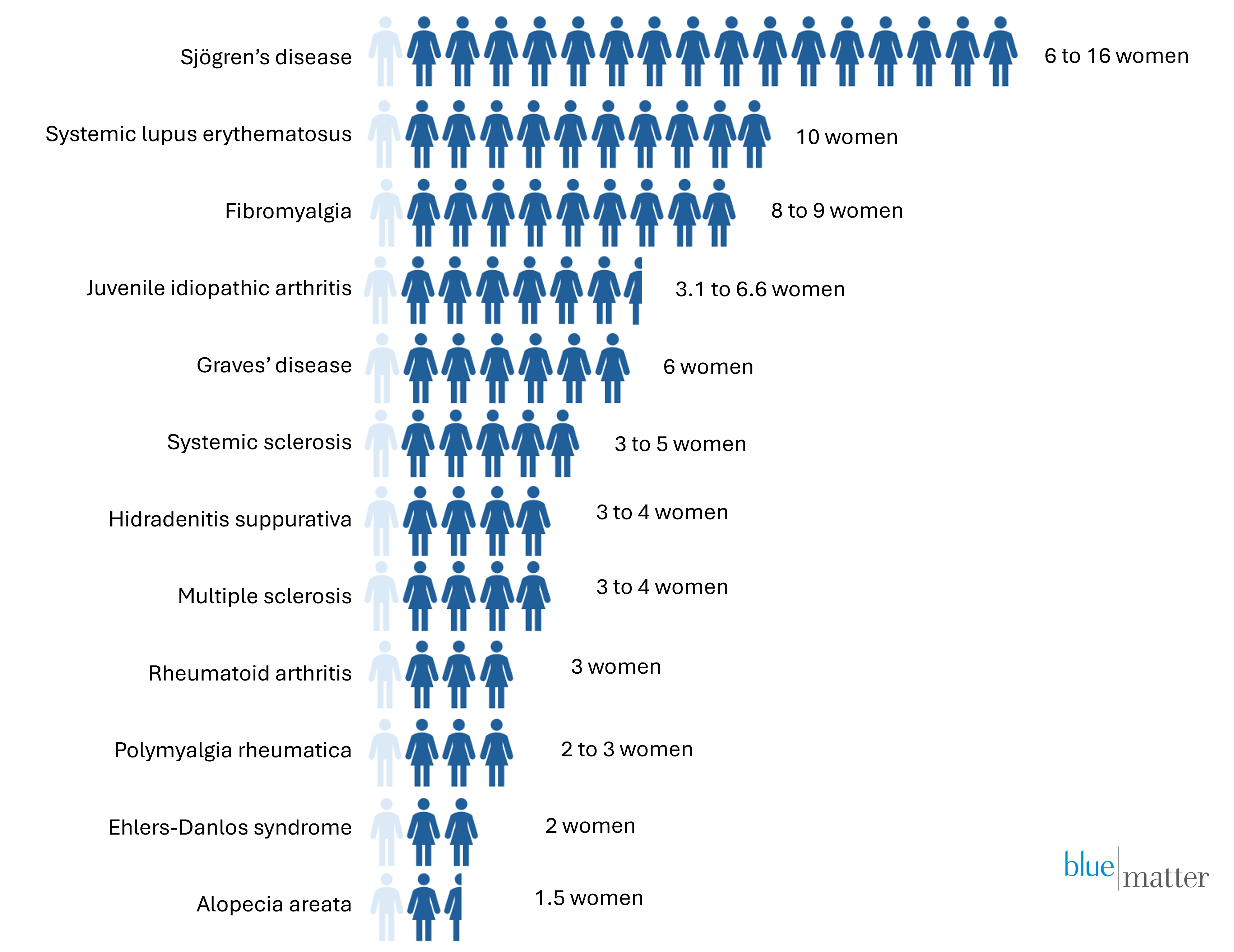
Greater Prevalence: Some diseases are far more prevalent in women (see Figure 1 below), and this can start early in the patient’s life. For example, more than 75% of juvenile idiopathic arthritis patients are girls[1]. There are many potential reasons for the prevalence differences, including genetics, hormone fluctuations, musculoskeletal variation, and autoantibodies to the long non-coding RNA responsible for inactivation of one X chromosome in women.[2]
Increased Severity: Other autoimmune and inflammatory diseases have similar prevalence across genders, but have different and frequently more severe symptomology, as well as a greater overall burden of disease in women. Rheumatoid arthritis, for example, tends to be more severe in women; they frequently experience higher numbers of tender or swollen joints and greater pain and fatigue.[3]
Figure 1: Gender Prevalence Differences (Number of Female Patients for Every Male Patient)
In recent years, awareness of the impact that autoimmune and inflammatory diseases have on women has been rising. As a result, we are seeing more basic research on the pathophysiology and presentation of these diseases in women, and more funding has been going into drug development for these types of diseases. As an example, the inflammatory component of endometriosis has only recently been elucidated, and much more research is needed, but programs in development now include Roche / Chugai’s IL-8 recycling mAb and several mPGES-1 inhibitors. These potential future therapies target inflammatory pathways, rather than the hormone receptors targeted by current treatments.
This growing focus on autoimmune and inflammatory disease in women presents opportunities for companies in the space. Some of the key implications across the development lifecycle include:
- Therapeutic Area Strategy: With the increased scientific understanding of inflammation and autoimmunity, there are now opportunities to target diseases that have seen limited investment in the past, and to focus more attention on areas where drug development has been challenging or high-risk. Many of these diseases, such as fibromyalgia, have very high unmet need and few treatment options, offering a first-mover advantage for companies willing to invest and build the future market.
- Funding: For privately-funded companies in particular, institutions and investors with a focus on women’s health may have an interest in investing in autoimmune and inflammatory diseases that disproportionately affect women. Despite challenges within the landscape, funding has been growing. In 2024, US investment in diseases that only or disproportionately affect women is estimated to have reached $10.7 billion.[4]
- Clinical Evidence Planning: In diseases that disproportionately affect women, the clinical trial population is likely to reflect that dynamic with or without enrolment quotas set for women. However, ensuring that trials are attractive to female patients is key. For diseases that impact pre-menopausal women—and particularly those that impact fertility and pregnancy (e.g. systemic lupus erythematosus, which increases the risk of pregnancy loss)—companies must plan to invest in safety studies early in development and work with regulators to address the need for effective treatments in pre-menopausal women as early as possible at launch. Additionally, where symptoms and burden of disease differ between genders, companies must ensure that gender cohorts within trials are sufficiently powered to enable effective post-hoc analyses in men and women, and that endpoints, particularly patient-reported outcomes, accurately measure the holistic burden of disease for both women and men.
- Commercialisation: Even in today’s healthcare environment, women are more likely than men to have their symptoms ignored or misdiagnosed by doctors. Building disease awareness and referral pathways early, ahead of launch, will be key to support patient access to specialist treatment as early as possible in their journey and to address diagnosis gaps. In particular, some inflammatory diseases are progressive and may lead to very severe or irreversible disease states such as fibrosis (e.g. in systemic sclerosis). Patients will need to receive therapies targeting inflammatory pathways sufficiently early in their disease course for those therapies to be effective, making early diagnosis and intervention key. Including women’s health specialists in market building efforts can also help (e.g. in hidradenitis suppurativa, where many patients are diagnosed and treated by gynaecologists as well as dermatologists).
The annual meeting of EULAR (the European Alliance of Associations for Rheumatology) is coming up in Barcelona, from 11-14 June. We are looking forward to seeing the latest presentations and data from companies focused on autoimmune and inflammatory diseases, particularly those that disproportionately affect women, as the unmet need in that segment is very high. We will be sure to stay abreast of the latest developments and bring those to you. Look out for a summary of key highlights from EULAR to come later in June. In the meantime, be sure to check our Insights page frequently or follow us on LinkedIn to see our latest publications.
End Notes:
[1] Cattalini M, Soliani M, Caparello MC, Cimaz R. Sex Differences in Pediatric Rheumatology. Clin Rev Allergy Immunol. 2019 Jun, : https://pubmed.ncbi.nlm.nih.gov/28849549/
[2] Goldman, Bruce, Stanford Medicine-led study shows why women are at greater risk of autoimmune disease, Stanford Medicine, Feb. 1, 2024, https://med.stanford.edu/news/all-news/2024/02/women-autoimmune.html
[3] Sokka T et al. Women, men and rheumatoid arthritis: analyses of disease activity, disease characteristics, and treatment in the QUEST-RA study. Arthritis Res. Ther., 2009. https://pubmed.ncbi.nlm.nih.gov/19144159/
[4] Silicon Valley Bank 2025 Innovation in Women’s Health Report, https://www.svb.com/news/company-news/venture-capital-investment-in-womens-health-startups-reaching-record-highs–silicon-valley-bank-releases-report/
Sources for Figure 1:
Sjogren’s (https://pmc.ncbi.nlm.nih.gov/articles/PMC4630965/)
SLE (https://pmc.ncbi.nlm.nih.gov/articles/PMC3605704/)
Fibromyalgia (https://openrheumatologyjournal.com/VOLUME/18/ELOCATOR/e18743129356140/FULLTEXT/)
JIA (https://pubmed.ncbi.nlm.nih.gov/28849549/)
Graves’ disease (https://pubmed.ncbi.nlm.nih.gov/21605717/)
MS (https://www.webmd.com/multiple-sclerosis/ms-affects-women-more-than-men)
RA (https://www.webmd.com/rheumatoid-arthritis/ra-and-women)
Ehlers-Danlos (https://www.ehlers-danlos.org/news/new-research-shows-heds-and-hsd-10-times-more-common-than-previously-thought/)
AA (https://jamanetwork.com/journals/jamadermatology/fullarticle/2801704 )