Rare vs. Specialty Diseases: Are They the Same?
We’ve often been asked what the differences are between rare diseases and “specialty diseases” and/or rare cancers. After all, these three types of disease share some similar characteristics. For example, they’re often complex, require higher-cost and “higher touch” treatments, and a high degree of knowledge and specialization. Related to this, some have even asked whether—from a biopharmaceutical company standpoint—this is all just forcing a distinction without any real difference.
The truth is, rare diseases (RDs) differ from specialty diseases and rare oncology indications in a number of important ways. These differences translate into specific corresponding challenges that companies must address to successfully develop and commercialize products in the RD arena.
In this article, we examine the key attributes that differentiate RDs from specialty diseases and rare oncology indications. We also outline some key implications for any company that wants to bring novel treatment options to RD patients.
Key Differences
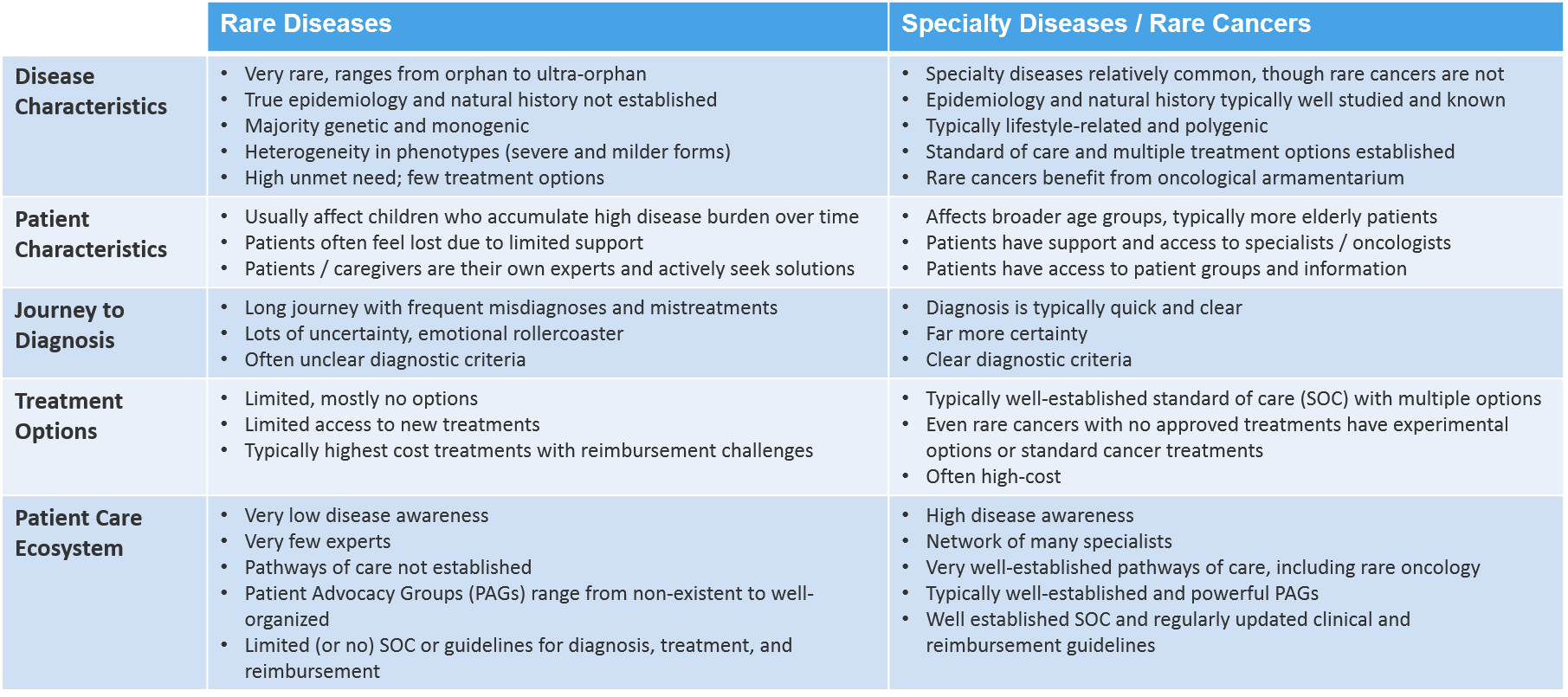
Rare diseases differ from specialty diseases and rare oncology indications in a range of different and meaningful ways. Below, we explore those differences in five key dimensions:
- Disease Characteristics
- Patient Characteristics
- Journey to Diagnosis
- Treatment Options
- Patient Care Ecosystem
Disease Characteristics
Obviously, orphan and ultra-orphan diseases are quite rare and most of them are not well studied. As a consequence, the true epidemiology has not been established for most rare diseases. The natural history of any given RD is not usually known and also remains to be established.
Most RDs are of genetic origin (mostly monogenic, meaning that a single gene is typically implicated in the disease process). As a result, RDs typically manifest early in life and mostly affect young children. However, due to genetic disease heterogeneity, milder forms of many RDs can also occur later in life and in adults.
Importantly, the vast majority of RDs do not have an approved treatment option. Hence, there is typically a very high level of unmet need.
In contrast, specialty diseases are much more common. Their epidemiology and natural histories are usually quite well studied and established. Largely caused by lifestyle factors, specialty diseases are typically of polygenic origin, meaning that the disease mechanism involves the combined action of multiple genes.
With specialty diseases, a standard of care is generally well-established. Patients usually have access to multiple treatment options that are approved and available. And, while there are exceptions, rare cancers are generally much better studied and characterized than non-oncological RDs. The very significant biopharmaceutical focus on oncology clearly has beneficial spill-over effects for rare oncological conditions.
Patient Characteristics
Patients with RDs will often experience the most dramatic differences when compared with those who suffer from more common specialty or rare oncology indications. A hallmark of RDs is that—due to their typically genetic origin—they disproportionally affect newborns, infants, and children. That makes early diagnosis, patient care, and therapeutic intervention very challenging.
Sadly, many children die of their rare condition at a very young age. Those individuals with a milder form of the disease who live longer will accumulate a very high disease burden as their condition progresses over time.
Specialty diseases and rare cancers can also affect children. However, these conditions generally and disproportionally affect adults and older patients.
Journey to Diagnosis
RD patients and their caregivers often experience very long, emotionally challenging journeys with significant uncertainty until a diagnosis is even suspected. On average, it can take many years, numerous visits to different doctors and specialists, and even multiple misdiagnoses and wrong treatments until a definitive diagnosis is established.
The patient burden of the long and winding journey to diagnosis is substantial. This often leaves patients and their caregivers with a feeling of being lost with no one to help them. This situation often forces these patients and their caregivers to become their own disease experts and to drive their own solutions.
This situation is usually quite different for patients with diseases that are treated by specialists. Typically, these patients are quickly referred from primary care doctors to disease specialists and receive a diagnosis in short order. Even patients with a rare oncology condition or a tumor will quickly be pointed towards oncologists who will be able to establish a diagnosis in a short time. The journey is generally much shorter with a lot less uncertainty. That doesn’t make the disease any less serious, but at least the patient can more quickly learn what he or she is dealing with and move more decisively into treatment.
Treatment Options
Probably the most dramatic difference for patients with RDs is the general lack of treatment options. Even if RD patients have their conditions eventually—and after an arduous journey—diagnosed, they will often find that there is nothing doctors can do to treat their disease.
Only a small fraction of all RDs—about 5%—have an approved treatment. And even for the few RDs with an approved treatment, therapies are typically very expensive, making broad access and reimbursement another challenge.
In contrast, patients with specialty conditions have access to a broader set of established and effective treatment options. Due to much higher patient numbers, these treatments are much more affordable and reimbursed with few restrictions.
Of course, there are rare cancers with no approved treatments. However, even for those there are usually viable treatment options such as surgery, radiation, and approved treatments from other oncological conditions with similar mutations that can be used off-label. In addition, there are a lot more treatment options approved or in development for rare cancers than for most other rare diseases.
Patient Care Ecosystem
The “ecosystem” of all players involved in providing care for RD patients differs from that of other diseases, too. Here, we take a quick look at that patient care ecosystem and its characteristics.
Health Care Providers and Centers of Care
Given the large number of RDs—around 7,000—and the very low number of approved treatments, it is unsurprising that there are very few experts for a particular RD. The basic levels of awareness for any given RD is generally quite low.
As the level of expertise and awareness is low, there are also very few centers that can provide specialized care for RD patients. This is probably the main reason why RD patients feel isolated and why getting an accurate diagnosis can take so long.
This is in stark contrast to the situation facing patients with more common specialty conditions. Disease awareness, even at the level of general practitioners, is generally much higher and the referral pathways from primary to specialty care are very well-established. This results in relatively fast diagnosis and treatment.
Even patients with rare cancers will quickly turn to established and usually well-resourced oncology centers that will do their best to rapidly establish a diagnosis and come up with potential treatment options. As mentioned above, even if there is no approved treatment for a given rare cancer condition, there is still the classical oncological treatment armamentarium, as well as potential off-label options for tumors with related pathophysiologies or genetic abnormalities.
Patient Organizations
Due to very low patient numbers and the lack of disease awareness, patient organizations for particular RDs are generally rudimentary or not developed at all. While there are RD umbrella organizations such as the National Organization for Rare Disorders (NORD) in the US and Eurordis in Europe, they have the challenge of organizing information and resources for thousands of diseases, which can result in a relatively low priority for certain if not most RDs.
This situation is dramatically different for a few rare disease ‘hot-spots’ such as spinal muscular atrophy (SMA) and Duchenne muscular dystrophy (DMD). Fortunately, patients with those diseases now have access to well-developed, well-funded, and powerful patient organizations. These have typically been driven by determined caregiver and parent networks that were also supported by biopharmaceutical companies which had developed treatment options for these conditions.
The SMA and DMD examples are rare and the exceptions in the RD space. However, they are quite typical when it comes to the more common specialty conditions. Patient organizations for specialty diseases are generally very well organized, often in a highly professional manner, receive excellent funding, and are highly influential. A similar situation is true for rare oncological disorders. There are very strong and well-organized international and national cancer organizations, often even organ-specific (e.g. breast or lung cancer).
Disease Policy and Treatment Guidelines
Due to a lack of strong patient organizations and weak or non-existing advocacy for most rare diseases, there is generally a lack of public policy focus and very few efforts to establish the best level of care for these diseases. With very few approved RD treatments and therapeutic options—and a general lack of well-established diagnostic criteria—there are very few recognized diagnostic, treatment and reimbursement guidelines.
This again is dramatically different for the much more common specialty diseases. Strong and well-organized patient organizations will forcefully drive public policy and disease priority leading to improved care, awareness, and broad patient access to affordable and effective treatments. Rare cancer conditions are supported by the existing strong oncology associations and generally benefit from the powerful policy focus of established cancer groups.
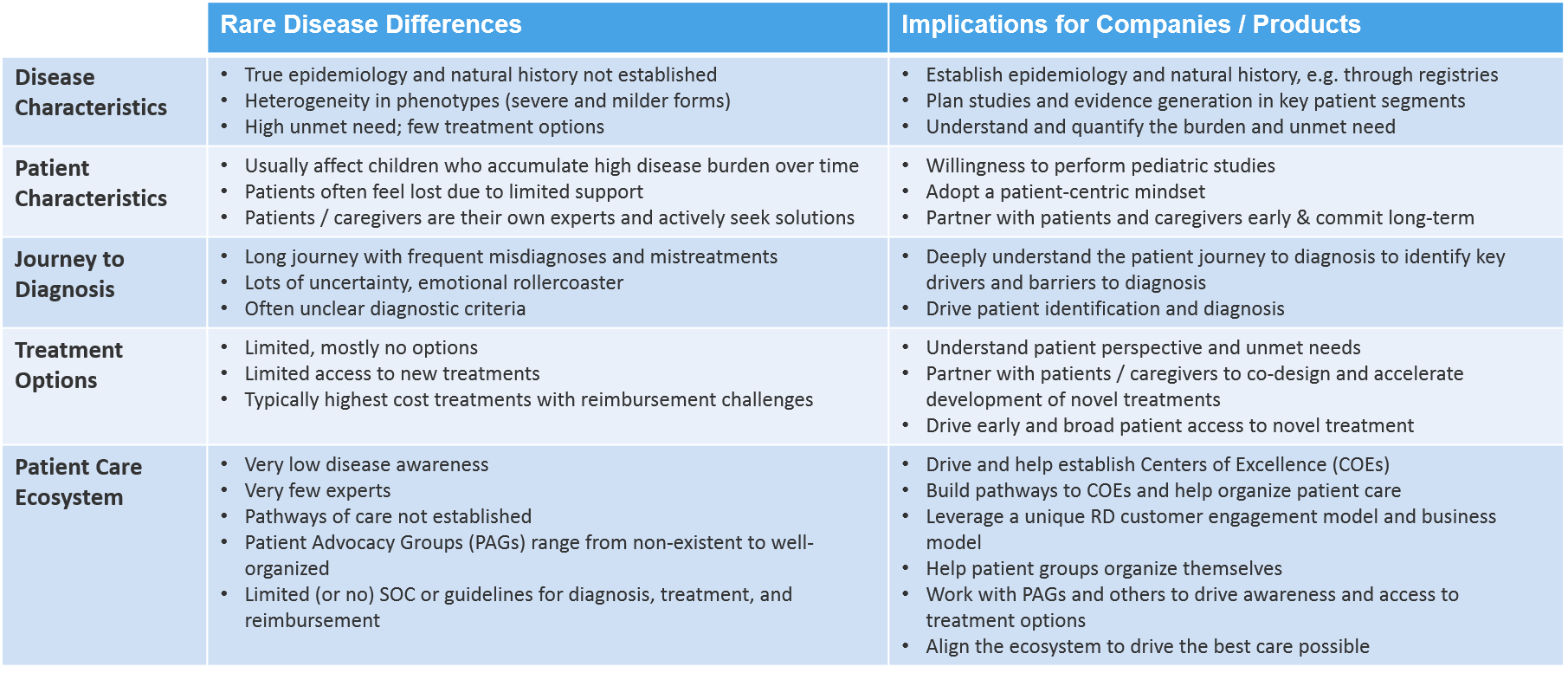
Implications for RD Companies
Most of the differences described above have major implications for companies operating in the RD space. Commercializing RD therapies requires a very different mindset and a special set of skills, tools, and capabilities. Below, we’ll introduce some of the key considerations for RD commercial strategists.
Characterization of Novel Rare Diseases
For a company who wants to develop a novel treatment for an RD with no existing treatment option, it’s absolutely critical to understand the true epidemiology and the natural history of the disease as soon as possible. A clear understanding and mapping of the different patient segments (e.g., by age and disease severity, as well as patient numbers by segment), will help to prioritize and select the most appropriate patients. In parallel, gaining a deep understanding of the unmet need and quantifying the disease burden will aid prioritization efforts and guide future efforts.
Patient Centricity
Patient focus and true “patient centricity” are core to the RD mindset. Patients and their caregivers will often have unparalleled knowledge of their condition so that they become and act like their own experts. They become highly involved and influential in making treatment decisions. An RD company must adopt a mindset that is uniquely and relentlessly focused on the patient and that puts the patient firmly in the center of everything it does.
The most successful and respected RD companies have developed early, trusting, and long-lasting relationships with patient groups by partnering with them and making substantial long-term commitments. These partnerships are critical to understand, unravel, and quantify patient needs. Understanding patient needs will help to design the most robust clinical studies, select the most patient-relevant clinical endpoints, and help generate high-value treatments with robust clinical and economic evidence.
As RDs mostly affect children, companies must be prepared to conduct and commit to pediatric studies which represents a challenge in itself.
In addition, trusting patient partnerships are also key to mapping the major obstacles and drivers to patient diagnosis, and designing the most effective strategies for patient identification. Obviously, patient identification is a critical factor in determining disease epidemiology, the feasibility and speed of study enrollment, and—ultimately—the commercial viability and success of a novel RD treatment option.
Aligning the RD Patient-Care Ecosystem
A company entering the field of rare diseases should be prepared to play a major role in aligning all players that are involved in providing care to patients with a particular rare disease. The ultimate goal should be to align the ecosystem in a way that provides the best and most effective care possible for the disease in question.
Doing this starts with a thorough understanding of patients’ perspectives and needs. However, it also must include the perspectives and needs of disease experts and treaters, regulators, payers, and other critical ecosystem partners. By taking all of these into account, a company has the potential to dramatically shortcut the time to bring a novel innovative treatment option to patients.
There are other critical components in aligning the ecosystem. These can include establishing dedicated and highly specialized centers of RD care, as well as building and organizing the patient pathways from primary care to these centers. An RD company can also help empower patients and patient groups to organize themselves so that they can drive disease awareness, influence policy efforts and guidelines, and establish broad and early access to a novel treatment option.
The RD mindset helps drive the unique RD business model. The most successful RD companies are committed for the long-haul, becoming deeply emotionally invested in the conditions they seek to treat. This unique model adopts a patient-centric attitude, helps align the patient care ecosystem, and partners with a range of stakeholders to achieve the ultimate goal of providing the best care for RD patients possible.
Summary and Conclusion
There are substantial and significant differences between rare and more common diseases, including rare oncological diseases.
The most obvious difference is the very low number of patients with any given rare disease (and the corresponding rarity of RD experts and treaters). Another key difference is the kind of patients that typically have an RD. Given the genetic origin of most RDs, newborns, infants and children are disproportionally affected.
As a direct consequence of the rarity describe above, disease priority and awareness are low. Most RDs remain without effective approved treatments. Patients with RDs often face an unusually high disease burden and have a long and emotionally challenging journey until their disease is diagnosed. With few established centers of care and too few treatment options, RD patients often feel isolated and desperate.
All of these differences have meaningful implications for companies that operate in the RD space. Any company that wants to bring a new RD therapy to market (and also succeed from a commercial standpoint) must understand these differences and be able to work within a universe in which these RD-specific challenges are the norm. Those companies that can align the RD ecosystem around patients’ needs and help to effectively organize patient care have a huge opportunity to create value and will make a profound difference for patients with rare diseases.